









Rezistența la insulină: ghid complet — cauze, simptome, HOMA, alimente și tratament
Rezistența la insulină este una dintre cele mai răspândite condiții metabolice ale momentului — și, paradoxal, una dintre cele mai puțin diagnosticate. Începe silențios, cu oboseală inexplicabilă și pofte de dulce la 3 după-amiaza, și poate evolua, dacă e ignorată, către prediabet și diabet de tip 2. Vestea bună: este una dintre puținele afecțiuni cronice complet reversibile prin alegeri conștiente. Acest ghid integrează tot ce trebuie să știi — de la mecanismul biologic, la indicele HOMA, la alimentele care îmbunătățesc sensibilitatea, la suplimentele cu impact dovedit.
Ce este rezistența la insulină și cum afectează organismul
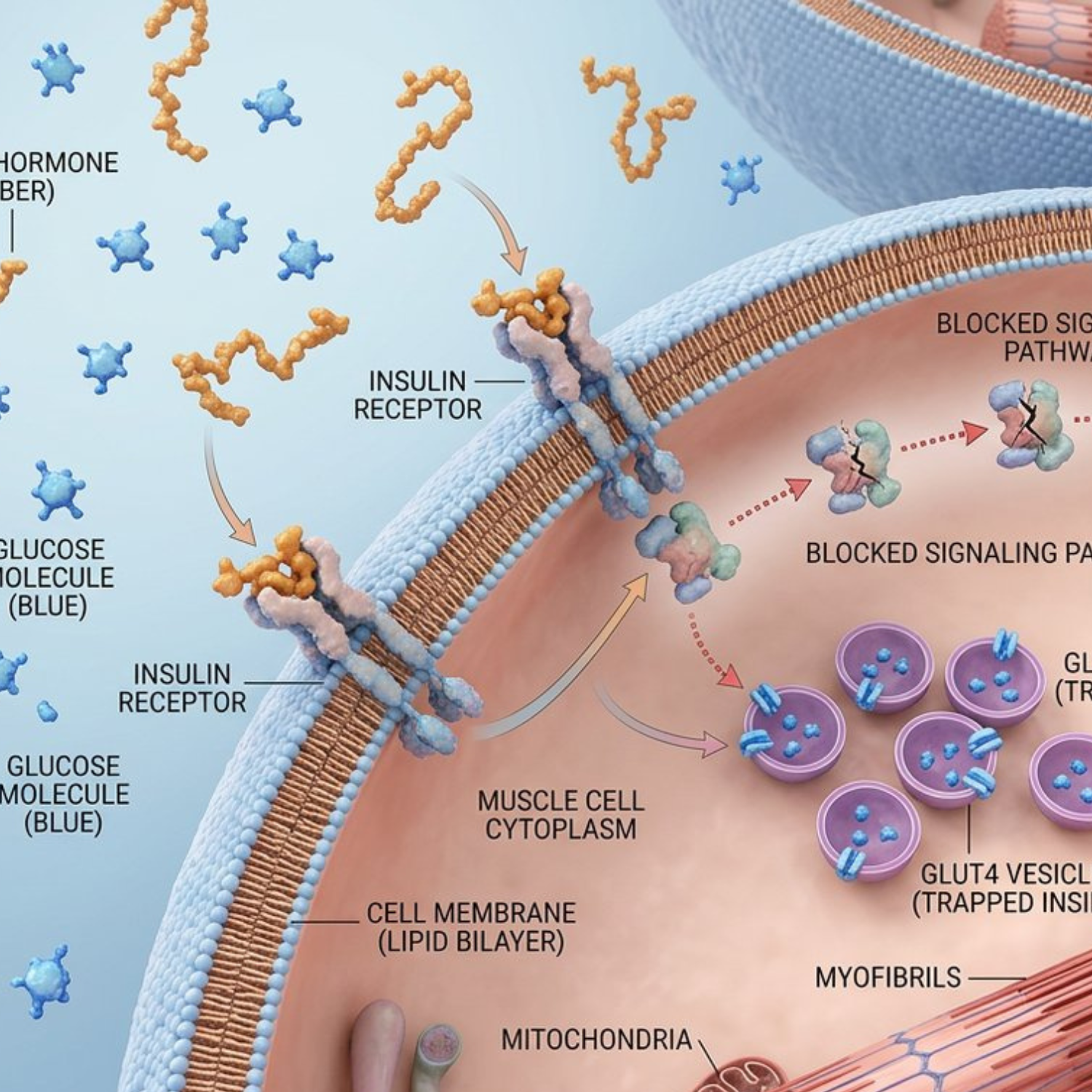
Rezistența la insulină este o stare în care celulele corpului — în special cele din mușchi, ficat și țesutul adipos — nu mai răspund eficient la acțiunea insulinei. Insulina este un hormon produs de pancreas cu un rol fundamental: facilitează intrarea glucozei din sânge în celule, unde aceasta este transformată în energie. Când acest mecanism funcționează corect, glicemia rămâne stabilă, iar metabolismul lucrează în echilibru.
Când apare insulinorezistența, celulele ignoră practic semnalul hormonal. Pancreasul detectează că glucoza nu este absorbită corespunzător și răspunde prin producerea unor cantități tot mai mari de insulină. Această suprasolicitare continuă duce la hiperinsulinemie — nivel cronic crescut de insulină în sânge — care, în timp, epuizează capacitatea pancreasului de a compensa. Rezultatul poate fi prediabetul și, ulterior, diabetul de tip 2.
Dincolo de glicemie, insulina mare pe termen lung perturbă alte procese metabolice: favorizează acumularea de grăsime abdominală (viscerală), dezechilibrează hormonii feminini și crește riscul cardiovascular. Afecțiunea evoluează lent, adesea fără simptome evidente în fazele incipiente — iar acest caracter silențios o face deosebit de periculoasă.
Sensibilitatea la insulină este opusul rezistenței: cu cât celulele tale răspund mai bine la insulină, cu atât ai nevoie de cantități mai mici din acest hormon pentru a menține glicemia în limite normale. Restabilirea sensibilității este obiectivul oricărei strategii metabolice — și e absolut posibilă, indiferent de vârstă.
Sindromul metabolic și legătura cu rezistența la insulină
Rezistența la insulină rareori apare izolat. Se află, de cele mai multe ori, în centrul unui ansamblu clinic numit sindrom metabolic — un grup de tulburări care apar simultan și care, împreună, cresc semnificativ riscul de boli cardiovasculare, accident vascular cerebral și diabet de tip 2.
Criteriile de diagnostic pentru sindromul metabolic includ:
- Obezitate abdominală — circumferința taliei peste 88 cm la femei și 102 cm la bărbați
- Hipertensiune arterială — tensiune peste 130/85 mmHg
- Trigliceride crescute — peste 150 mg/dL
- Colesterol HDL scăzut — sub 50 mg/dL la femei, sub 40 mg/dL la bărbați
- Glicemie a jeun ridicată — peste 100 mg/dL
Prezența a cel puțin trei dintre aceste criterii confirmă diagnosticul. Tulburările se instalează gradual, iar scăderea toleranței la glucoză este adesea primul semnal că lucrurile nu mai funcționează optim. Identificarea timpurie este esențială tocmai pentru că stadiul de prediabet este complet reversibil prin intervenții adecvate.
Cauze și factori de risc pentru rezistența la insulină
Mecanismele prin care se instalează rezistența la insulină sunt complexe și implică o interacțiune între predispoziția genetică și factorii de mediu. Nu există o cauză unică, ci o acumulare de influențe care, în timp, perturbă sensibilitatea celulară:
- Obezitate viscerală — grăsimea abdominală eliberează citokine inflamatorii care interferează direct cu semnalizarea insulinică
- Sedentarism — lipsa activității fizice reduce sensibilitatea musculară la insulină, amplificând efectele metabolice negative
- Dietă bogată în zaharuri rafinate și ultra-procesate — provoacă fluctuații repetate ale glicemiei și solicită constant pancreasul
- Vârsta — riscul crește semnificativ după 35-40 de ani, în special la femei în perimenopauză
- Istoricul familial — predispoziția genetică crește vulnerabilitatea
- Stresul cronic — cortizolul ridicat interferează direct cu semnalizarea insulinică și favorizează grăsimea abdominală
- Somnul insuficient sau fragmentat — chiar și o singură noapte sub 5 ore reduce sensibilitatea la insulină cu 25-30% în 24 de ore
- Fluctuațiile hormonale — scăderea estrogenului în perimenopauză reduce sensibilitatea celulară la insulină
Hiperinsulinemia rezultată nu este o cauză în sine, ci un semn că organismul încearcă să compenseze un dezechilibru deja instalat. Pentru femei, conexiunea cu fluctuațiile hormonale este deosebit de importantă — citește mai mult despre cum perimenopauza schimbă metabolismul.
Simptome și semne ale rezistenței la insulină
Una dintre particularitățile rezistenței la insulină este că, în stadiile timpurii, evoluează silențios. Nu există durere, nu există un semnal clar — și tocmai această absență a simptomelor evidente o face dificil de identificat fără analize de sânge.
Semnele timpurii la care să fii atentă:
- Oboseală persistentă care nu dispare după odihnă — celulele nu pot extrage eficient energie din glucoză
- Pofte intense de dulce sau carbohidrați, în special la 2-4 ore după mese
- Senzație de foame la scurt timp după masă — semn că glucoza nu intră eficient în celule
- Dificultăți de concentrare, „brain fog" după mese — în special după prânz
- Acumulare de grăsime abdominală, chiar și în absența unui exces ponderal general
- Acanthosis nigricans — zone de piele îngroșată și închisă la culoare la nivelul gâtului, axilelor sau pliurilor cutanate (semn dermatologic specific)
- Tag-uri cutanate (acrocordoame) — formațiuni mici, moi, pe gât sau subraț
- Cicluri menstruale neregulate sau sindrom ovarian polichistic (PCOS) — la femei
- Tensiune arterială borderline, valori care nu mai sunt „normale"
Dacă bifezi 3+ din aceste simptome, în special asociate cu factori de risc (vârstă peste 35, sedentarism, istoric familial), e momentul să faci analizele de sânge specifice.
Indicele HOMA — cum se calculează și se interpretează
Indicele HOMA (Homeostatic Model Assessment) este standardul clinic pentru evaluarea rezistenței la insulină. Se calculează printr-o formulă matematică simplă: insulina a jeun (μU/mL) × glicemia a jeun (mmol/L), totul împărțit la 22,5. Ambele măsurători se fac dimineața, pe nemâncate, după minim 8 ore de repaus alimentar.
| Valoare HOMA-IR | Interpretare |
|---|---|
| Sub 1,0 | Sensibilitate optimă la insulină |
| 1,0 - 2,5 | Normal |
| 2,5 - 3,5 | Rezistență la insulină incipientă |
| Peste 3,5 | Rezistență la insulină semnificativă |
Un HOMA-IR crescut nu este un verdict, ci un semnal care merită luat în serios și investigat în context clinic complet. Valoarea sa stă în ceea ce declanșează — schimbări de stil de viață, monitorizare, intervenții țintite — nu în cifra în sine. Analizele HOMA sunt utile nu doar pentru diagnostic, ci și pentru monitorizarea evoluției în timp și a răspunsului la intervenții.
Diagnostic complet — analize și teste necesare
Diagnosticarea rezistenței la insulină nu se bazează pe un singur test, ci pe o evaluare corelată a mai multor parametri biologici:
- Insulina a jeun și glicemia a jeun — permit calcularea HOMA-IR; valori optime: insulină < 10 μU/mL, glicemie < 100 mg/dL
- Hemoglobina glicată (HbA1c) — reflectă media glicemiei din ultimele 2-3 luni; normal sub 5,7%, prediabet 5,7-6,4%, diabet ≥ 6,5%
- Testul de toleranță la glucoză orală (TTGO) — măsurarea glicemiei înainte și la 2 ore după consumul a 75g glucoză; cel mai sensibil test pentru prediabet timpuriu
- Profil lipidic complet — colesterol total, LDL, HDL, trigliceride; relevant pentru sindromul metabolic asociat
- Tensiunea arterială și circumferința abdominală — parametri clinici esențiali
- Proteina C reactivă (CRP) ultrasensibilă — marker de inflamație sistemică, frecvent crescut în rezistența la insulină
Recomandarea este să faci aceste analize anual după 35 de ani, chiar dacă nu ai simptome — și mai des dacă bifezi factori de risc.
Alimentele care îmbunătățesc sensibilitatea la insulină
Alimentația este cel mai puternic instrument pe care îl ai. Principiul de bază: reduci solicitarea pancreasului limitând carbohidrații rafinați și zahărul adăugat, în timp ce construiești mesele în jurul alimentelor care stabilizează glicemia.
Alimente care reduc rezistența la insulină
Legume cu frunze verzi — spanac, kale, rucola — sunt printre cele mai valoroase pentru sănătatea metabolică, datorită conținutului ridicat de magneziu și fibre și indicelui glicemic extrem de scăzut. Broccoli, conopida, ardeii și dovleceii completează această categorie. Regula practică: cu cât leguma e mai colorată și mai puțin procesată, cu atât efectul asupra glicemiei e mai blând.
Cereale integrale — ovăzul, orezul brun, quinoa, orzul, hrișca — eliberează glucoza treptat, spre deosebire de variantele rafinate care provoacă creșteri rapide ale zahărului din sânge. Această eliberare lentă menține energia constantă și reduce semnificativ necesarul de insulină.
Leguminoase — fasole uscată, linte, năut, mazăre — surse excelente de proteine vegetale și fibre solubile. Studiile arată că includerea lor regulată (3-4 porții pe săptămână) contribuie la stabilizarea glicemiei și reducerea HOMA-IR cu 0,3-0,5 puncte după 8-12 săptămâni.
Proteine de calitate — pește gras (somon sălbatic, sardine, hering), pui fără piele, ouă, proteine vegetale combinate. Nu provoacă creșteri semnificative ale glicemiei, susțin masa musculară (care absoarbe glucoza fără insulină) și prelungesc sațietatea. Plant Protein de la Lunaawell oferă 25g proteină completă per porție, cu profil de aminoacizi optimizat pentru sațietate și recuperare metabolică.
Grăsimi sănătoase — avocado, nuci, semințe (in, chia, cânepă), ulei de măsline extra virgin. Contribuie la profilul lipidic și încetinesc absorbția carbohidraților.
Fructe cu indice glicemic scăzut — afine, zmeură, căpșuni, mere cu coajă, kiwi. Conțin polifenoli antioxidanți care îmbunătățesc direct sensibilitatea celulară la insulină.
Condimente cu impact metabolic — scorțișoară de Ceylon (½-1 linguriță zilnic), turmeric cu piper negru, ghimbir proaspăt. Toate au studii care arată reduceri ale glicemiei post-prandiale de 10-30%.
Alimente de evitat sau de redus drastic
La fel de important: să recunoști ce sabotează sensibilitatea la insulină. Alimentele cu indice glicemic ridicat provoacă creșteri rapide ale glicemiei și forțează pancreasul să răspundă cu valuri mari de insulină:
- Produse de patiserie și panificație din făină albă (pâine, baghete, croasante)
- Cereale procesate pentru micul dejun cu zahăr adăugat
- Dulciuri concentrate, prăjituri, bomboane
- Băuturi carbogazoase îndulcite și sucuri de fructe industriale
- Orez alb rafinat (în cantități mari)
- Paste din făină albă
- Alimente prăjite în uleiuri industriale (floarea-soarelui, soia, porumb)
- Alcool zilnic — perturbă reglarea glicemiei și a cortizolului
- Îndulcitori artificiali (sucraloza, aspartam) — pot afecta microbiomul și sensibilitatea la insulină chiar dacă nu cresc direct glicemia
Regim zilnic pentru prediabet și sensibilitate optimă la insulină
Un regim alimentar pentru sensibilitate la insulină nu trebuie să fie complicat, dar trebuie să fie consecvent. Structura zilei contează enorm: mesele regulate, la intervale aproximativ egale, previn fluctuațiile mari ale glicemiei.
Micul dejun optim
Prima masă a zilei stabilește „tonul metabolic" pentru orele următoare. Un mic dejun optim combină proteine + grăsimi sănătoase + fibre, evitând carbohidrații rafinați care provoacă spike-ul matinal de glicemie.
Exemple:
- Omletă cu 3 ouă + spanac + avocado + roșii cherry
- Iaurt grecesc cu fructe de pădure proaspete, nuci și semințe de chia
- Shake cu Plant Protein + semințe de in + afine + lapte de migdale
- Ovăz integral cu unt de migdale, scorțișoară și fructe de pădure
Prânz și cină
Construiește-ți farfuria după o regulă simplă: ½ legume + ¼ proteine slabe + ¼ cereale integrale sau leguminoase. Adaugă o sursă de grăsime sănătoasă (avocado, ulei de măsline, nuci) pentru a încetini absorbția carbohidraților.
Tactici suplimentare cu impact glicemic dovedit:
- Mănâncă proteinele + fibrele înainte de carbohidrați la fiecare masă — aplatizează curba glicemică cu până la 40%
- O lingură de oțet de mere în apă înainte de mese — sensibilizează receptorii de insulină
- Mers 10-15 minute după mese — reduce glicemia post-prandială cu până la 30%
Suplimente pentru rezistența la insulină — ce funcționează cu adevărat
Alimentația și mișcarea sunt fundația, dar anumite suplimente au studii clinice solide care arată impact măsurabil asupra rezistenței la insulină.
Cromul picolinat
Cromul joacă un rol direct în semnalizarea insulinică. Recomandarea EFSA confirmă: cromul contribuie la menținerea nivelurilor normale de glucoză în sânge. Chiar și o ușoară insuficiență de crom poate compromite eficiența cu care insulina își face treaba. Metabolic-R Glucose de la Lunaawell combină crom picolinat cu sinergici metabolici formulați specific pentru femei în perimenopauză.
Berberina
Una dintre cele mai bine studiate plante pentru sănătatea metabolică. Activează enzima AMPK — un „switch metabolic" identic cu cel activat de exercițiu și de metformin. Reduce gluconeogeneza hepatică, îmbunătățește absorbția glucozei în mușchi și modulează microbiomul. În unele studii clinice, efectele asupra HbA1c sunt comparabile cu cele ale metforminului.
Atenție: berberina interacționează cu medicamente pentru diabet (poate cauza hipoglicemie) și cu anticoagulante. Consultă medicul înainte de a o combina cu tratament medicamentos.
Magneziu glicinat
Deficiența de magneziu e extrem de frecventă la persoanele cu rezistență la insulină — iar suplimentarea îmbunătățește semnificativ sensibilitatea. Doza: 200-400 mg seara, forma glicinat pentru absorbție optimă și fără efect laxativ.
Acizi grași Omega-3 (EPA + DHA)
Reduc inflamația sistemică care interferează cu semnalizarea insulinică. Țintă: 1-2g EPA+DHA pe zi, dintr-un supliment de calitate sau 2-3 porții de pește gras pe săptămână.
Extract de scorțișoară
În special varianta Ceylon (nu cassia). Încetinește digestia carbohidraților și îmbunătățește sensibilitatea receptorilor de insulină. Doza: ½-1 linguriță zilnic în alimente sau 500-1000 mg extract standardizat.
Extract de ceai verde (EGCG)
Antioxidant cu impact asupra eficienței mitocondriale și a inflamației de fundal. Susține metabolismul și sensibilitatea la insulină. Doza: 300-500 mg EGCG zilnic.
Oțet de mere
Studii mici arată reducerea răspunsului glicemic post-prandial cu 20-30% când e consumat (1 lingură în apă) cu 10-15 minute înainte de mesele cu carbohidrați.
Activitate fizică — cel mai eficient „medicament" natural
Exercițiul fizic este unul dintre cele mai puternice instrumente împotriva insulinorezistenței. Când mușchii se contractă, ei pot absorbi glucoza din sânge independent de insulină — un mecanism care reduce direct glicemia și, în timp, îmbunătățește sensibilitatea celulară.
Combinația optimă:
- Exerciții aerobice moderate — mers alert, ciclism, înot — 30-45 minute, 4-5 zile pe săptămână
- Antrenament de forță — 2-3 sesiuni de 30-40 minute pe săptămână, mișcări compuse (squat, deadlift, push-up, row)
- HIIT scurt — 1-2 sesiuni de 15-20 minute pe săptămână, pentru stimul mitocondrial
- NEAT (mișcare neasociată exercițiului) — pauze de 2-3 minute la fiecare oră de șezut, mers după mese
Antrenamentul de forță e deosebit de important după 35 de ani: mușchii pierduți natural (sarcopenie) reduc capacitatea bazală de absorbție a glucozei. Conservarea masei musculare este una dintre cele mai puternice intervenții împotriva rezistenței la insulină pe termen lung.
Somn, stres și factori lifestyle subestimați
Somnul și gestionarea stresului sunt adesea ignorate, dar au impact direct asupra rezistenței la insulină. O singură noapte de somn fragmentat reduce sensibilitatea la insulină cu 25-30% în 24 de ore. Stresul cronic crește cortizolul, care interferează direct cu semnalizarea insulinică și favorizează grăsimea viscerală.
Strategii cu impact:
- Somn 7-8 ore în cameră răcoroasă (18-19°C), fără lumini și fără telefon
- Magneziu glicinat seara pentru somn profund
- Mâncare ultimă cu minim 3 ore înainte de somn
- Tehnici de respirație (box breathing, 4-7-8) pentru cortizol acut
- Expunere la lumină naturală în primele 30 minute după trezire
Citește mai mult despre legătura cortizol → rezistență la insulină → grăsime abdominală.
Tratament medicamentos — când este necesar
În multe cazuri, modificările de stil de viață sunt suficiente pentru a inversa traiectoria metabolică. Dar uneori, mai ales când HOMA-IR e foarte ridicat (peste 5) sau când prediabetul a evoluat spre diabet, medicul poate recomanda intervenție medicamentoasă.
Metformina este cel mai frecvent utilizat medicament. Reduce producția hepatică de glucoză, îmbunătățește sensibilitatea musculară la insulină și are profil de siguranță bine documentat după zeci de ani de uz clinic. E adesea folosită chiar și off-label pentru sindrom ovarian polichistic sau pentru longevitate metabolică în cazuri selectate.
Alte clase de medicamente (GLP-1 agoniști, SGLT-2 inhibitori) pot fi indicate în prezența diabetului instalat sau a obezității severe — decizia aparține medicului. Pentru o perspectivă naturală asupra stimulării GLP-1, citește ghidul de stimulare a GLP-1 prin alegeri zilnice.
Monitorizarea pe termen lung
Sensibilitatea la insulină nu se „repară" o dată și apoi rămâne. Necesită monitorizare și ajustare în timp:
- HbA1c la fiecare 3-6 luni — cel mai bun indicator al evoluției
- HOMA-IR anual — pentru a vedea progresul
- Glicemia bazală lunar, dacă ești în stadiul de prediabet
- Profil lipidic anual — TG/HDL ratio e un marker excelent de sensibilitate
- Circumferința taliei măsurată acasă lunar — semnal timpuriu de evoluție bună sau slabă
Întrebări frecvente
Cât timp durează să-mi îmbunătățesc sensibilitatea la insulină?
Schimbările acute (poftele, energia post-meal) se simt în 2-3 săptămâni. Markerii (HOMA-IR, glicemia) încep să se îmbunătățească în 6-8 săptămâni de protocol consistent. Reducerea semnificativă a HbA1c necesită 3-6 luni. Femeile în perimenopauză pot vedea răspuns ceva mai lent — este normal, nu o eșec.
Trebuie să tai complet carbohidrații?
Nu. Carbohidrații complecși (cartof dulce, ovăz, leguminoase, fructe cu pulpă) sunt benefici și susțin tiroida, somnul și nivelurile sănătoase de cortizol. Ce trebuie să elimini sunt carbohidrații rafinați (pâine albă, paste, biscuiți, dulciuri) și să consumi carbohidrații complecși după proteine și fibre.
Pot inversa prediabetul fără medicamente?
În cele mai multe cazuri, da — studiile pe programe lifestyle (Diabetes Prevention Program) au arătat reducere de 58% a riscului de progresie la diabet doar prin alimentație, mișcare și pierdere modestă de greutate (5-7% din greutatea corporală). Medicația devine relevantă când lifestyle-ul nu e suficient sau când stadiul e mai avansat.
Care e cea mai bună analiză pentru a diagnostica rezistența la insulină devreme?
Combinația HOMA-IR (insulina + glicemia a jeun) + HbA1c oferă cea mai bună imagine timpurie. Glicemia a jeun singură ratează multe cazuri de rezistență — insulina a jeun ridicată poate apărea cu ani înainte ca glicemia să crească.
Sunt suplimentele necesare sau pot face totul prin alimentație?
Alimentația și mișcarea sunt fundația. Suplimentele țintite (crom, magneziu, omega-3, eventual berberină) sunt acceleratori care fac diferența între rezultate lente și rezultate vizibile, dar nu înlocuiesc lifestyle-ul. Discută cu medicul tău înainte de a începe orice supliment, mai ales dacă urmezi tratament medicamentos.
Concluzia care contează
Rezistența la insulină nu e o sentință — e un semnal. Îți spune că biologia ta cere o recalibrare, nu o restricție. Spre deosebire de multe afecțiuni cronice, asta e una dintre puținele unde intervențiile lifestyle au impact real și măsurabil, nu în săptămâni, ci în luni de consecvență.
Femeile care își apără masa musculară, își reglează glicemia prin alegeri alimentare conștiente, dorm protejat, gestionează stresul și își monitorizează markerii metabolici pot inversa complet rezistența la insulină — chiar și după 40, chiar și în perimenopauză. Nu cu efort eroic, ci cu obiceiuri sustenabile, construite zi de zi.
Corpul tău nu te trădează. Are nevoie doar de claritate, sprijin și răbdare consistentă.
Notă: Acest articol are scop educațional și nu înlocuiește consultul medical. Rezistența la insulină și prediabetul necesită evaluare individualizată. Înainte de a începe orice protocol de suplimentare sau dietă, mai ales dacă urmezi tratament medicamentos sau ai o afecțiune diagnosticată, consultă medicul tău.
Ți s-a părut util? Distribuie-l mai departe.
Distribuie pe InstagramCitește mai mult

Ce sunt antioxidanții și ce înseamnă pentru sănătate? Există un moment în viața fiecăruia dintre noi când începem să ne întrebăm cu adevărat ce punem în corpul nostru și de ce. Orice...

Corpul tău produce hormonul pe care Ozempic îl mimează. Cum stimulezi GLP-1 natural prin proteină, fibre, polifenoli și suplimente țintite — fără injecții, fără efecte adverse.

